

The Liver as an Organ
Although we do not consciously feel our liver working, it actually performs many important functions that are necessary for the maintenance of homeostasis. From blood storage to vitamin synthesis, the liver does so many things that in times of dysfunction, such as in drug-induced liver damage, the consequences immediately become apparent.

Anatomy of the liver
The liver is an organ in the upper right-hand part of your abdomen. It sits under the diaphragm, and on top of the stomach, right kidney, and intestines.
The liver is a dark reddish-brown color, and is shaped a bit like a wedge. It weighs about 3 pounds. The liver has 2 lobes. Both are made up of 8 segments that have of 1,000 small lobes called lobules. These lobules are connected to small tubes (ducts) that lead to larger ducts that form the common hepatic duct. The common hepatic duct sends the bile made by the liver cells to the gallbladder and the first part of the small intestine (duodenum) through the common bile duct.
The liver holds about 1 pint (13%) of your body's blood supply. There are 2 blood vessels that send blood to the liver. They are:
-
Hepatic artery. This sends oxygen-rich blood to the liver.
-
Hepatic portal vein. This sends nutrient-rich blood to the liver.
The liver is a dark reddish-brown color, and is shaped a bit like a wedge. It weighs about 3 pounds. The liver has 2 lobes. Both are made up of 8 segments that have of 1,000 small lobes called lobules. These lobules are connected to small tubes (ducts) that lead to larger ducts that form the common hepatic duct. The common hepatic duct sends the bile made by the liver cells to the gallbladder and the first part of the small intestine (duodenum) through the common bile duct.
Hepatic artery. This sends oxygen-rich blood to the liver.
Hepatic portal vein. This sends nutrient-rich blood to the liver.
Functions of the liver
The liver has more than 500 vital functions. All the blood leaving the stomach and intestines passes through the liver. The liver processes this blood. It breaks down, balances, and creates nutrients. It also processes medicines and other chemicals. The liver:
- Makes bile, which helps carry away waste and break down fats in the small intestine during digestion
- Makes certain proteins for blood plasma
- Makes cholesterol and proteins to help carry fats through the body
- Converts excess glucose into glycogen for storage and makes glucose as needed
- Controls blood levels of amino acids, which are the building blocks of proteins
- Processes hemoglobin for its iron and then stores the iron
- Converts ammonia to urea, which is then excreted in urine
- Clears medicines, drugs and other substances from the blood
- Controls blood clotting
- Helps prevent infections by making immune factors and removing bacteria from the blood
- Clears bilirubin from the blood
When the liver has broken down harmful substances, this waste is excreted into the bile or blood. Waste in bile enters the intestine and leaves the body in the form of feces. Waste in blood is filtered out by the kidneys, and leaves the body in the form of urine.
PHYSIOLOGY OF THE LIVER
The liver performs so many functions, which is why any disruptions in the integrity of the liver parenchyma result in drastic homeostatic changes which could only result to morbid or even fatal results if not controlled. An understanding of some of the features of the liver could shed light on how drugs bring about the signs and symptoms that are present in toxicities.
As a blood reservoir
The blood vessels in the normal adult liver can hold around 450 mL of blood during ordinary circumstances. However, because of its distensibility, it can hold up to 0.5 to 1 liter of blood in the presence of pathological conditions such as congestive heart failure or peripheral congestion. Because of this capability, the liver can store blood to normalize the pressure in the circulatory system and provide blood supply in situations where there is diminished blood supply.
Liver mass regulation
During partial liver resection, around 70 percent of the whole liver is removed. After this surgical procedure, the liver is able to regenerate a new set of hepatocytes and of course, regrow the lost portion of the organ. This amazing feature of the liver is thought to be a product of hepatocyte growth factor (HGF), epidermal growth factor, tumor necrosis factor (TNF) and interleukin 6 (IL-6). Although able to regenerate, the growth is limited to a certain extent with the help of transforming growth factor β (TGF-β)>.
The macrophage system
A large amount of blood normally flows through the sinusoids and into the liver parenchyma, which makes the liver very much prone to blood-borne infection and damage by pathogens and other substances. However, this is offset by the presence of the active phagocytosing Kupffer cells which constantly keeps pathogens from invading the liver tissue.
Macronutrient metabolism
The liver is the primary organ involved in the metabolism of carbohydrates, fats, and proteins. As for carbohydrates, the liver is responsible for the storage of glycogen and the formation of glucose units from other sources such as lipid and protein metabolites and other sugars. The liver is also responsible for the oxidation of fats and the synthesis of cholesterol and other lipids. For proteins, the organ is involved in the deamination and synthesis of amino acids.
Vitamin storage
The liver is very well known as a storage site for a lot of vitamins. The most dominant vitamins present in some of the hepatocytes in the liver are vitamin A, vitamin D and vitamin B12. With this feature, eating a diet that is low in the said vitamins for a few days does not necessarily lead to deficiencies. The liver is also an efficient storage site for iron.
The liver’s role in blood coagulation
There are many clotting factors that are produced in the liver. In the presence of vitamin K, the liver is able to synthesize fibrinogen, prothrombin, accelerator globulin, and factors VII, IX, and X.
The liver performs so many functions, which is why any disruptions in the integrity of the liver parenchyma result in drastic homeostatic changes which could only result to morbid or even fatal results if not controlled. An understanding of some of the features of the liver could shed light on how drugs bring about the signs and symptoms that are present in toxicities.
As a blood reservoir
The blood vessels in the normal adult liver can hold around 450 mL of blood during ordinary circumstances. However, because of its distensibility, it can hold up to 0.5 to 1 liter of blood in the presence of pathological conditions such as congestive heart failure or peripheral congestion. Because of this capability, the liver can store blood to normalize the pressure in the circulatory system and provide blood supply in situations where there is diminished blood supply.
Liver mass regulation
During partial liver resection, around 70 percent of the whole liver is removed. After this surgical procedure, the liver is able to regenerate a new set of hepatocytes and of course, regrow the lost portion of the organ. This amazing feature of the liver is thought to be a product of hepatocyte growth factor (HGF), epidermal growth factor, tumor necrosis factor (TNF) and interleukin 6 (IL-6). Although able to regenerate, the growth is limited to a certain extent with the help of transforming growth factor β (TGF-β)>.
The macrophage system
A large amount of blood normally flows through the sinusoids and into the liver parenchyma, which makes the liver very much prone to blood-borne infection and damage by pathogens and other substances. However, this is offset by the presence of the active phagocytosing Kupffer cells which constantly keeps pathogens from invading the liver tissue.
Macronutrient metabolism
The liver is the primary organ involved in the metabolism of carbohydrates, fats, and proteins. As for carbohydrates, the liver is responsible for the storage of glycogen and the formation of glucose units from other sources such as lipid and protein metabolites and other sugars. The liver is also responsible for the oxidation of fats and the synthesis of cholesterol and other lipids. For proteins, the organ is involved in the deamination and synthesis of amino acids.
Vitamin storage
The liver is very well known as a storage site for a lot of vitamins. The most dominant vitamins present in some of the hepatocytes in the liver are vitamin A, vitamin D and vitamin B12. With this feature, eating a diet that is low in the said vitamins for a few days does not necessarily lead to deficiencies. The liver is also an efficient storage site for iron.
The liver’s role in blood coagulation
There are many clotting factors that are produced in the liver. In the presence of vitamin K, the liver is able to synthesize fibrinogen, prothrombin, accelerator globulin, and factors VII, IX, and X.
Metabolism of Drugs in the Liver

Generally speaking, drugs are not the same when they are excreted out from the body (except for some). A lot of processes actually occur in between absorption and excretion, and this is mainly because of the metabolic features of the liver. In a phenomenon called the first-pass effect, medications and other substances that are absorbed in the gut are first transferred to the liver by the portal circulation. This makes the liver the screening area for the substances that enter the body through the digestive system.
Drugs undergo biotransformation in the liver in order to exist in the circulation in proper therapeutic amount and forms. Through this process, medications are also transformed into substances that are easily excreted in the urine and other excretory organs. It usually involves 2 phases:
- Phase I: Drugs are converted into more polar forms by adding functional groups.
- Phase II: Drugs that fail to become excreted after phase I are conjugated into more polar forms.
Without this function, toxic levels of the medications would remain in the bloodstream. Phase I reactions usually involve the microsomal protein CYP450 as well as other microsomal enzyme systems. Phase II usually involves conjugation reactions that are catalyzed by transferases. Substrates for these conjugation reactions usually include the endogenous substances glucuronic acid, sulfuric acid, acetic acid and some amino acids.

Generally speaking, drugs are not the same when they are excreted out from the body (except for some). A lot of processes actually occur in between absorption and excretion, and this is mainly because of the metabolic features of the liver. In a phenomenon called the first-pass effect, medications and other substances that are absorbed in the gut are first transferred to the liver by the portal circulation. This makes the liver the screening area for the substances that enter the body through the digestive system.
Drugs undergo biotransformation in the liver in order to exist in the circulation in proper therapeutic amount and forms. Through this process, medications are also transformed into substances that are easily excreted in the urine and other excretory organs. It usually involves 2 phases:
- Phase I: Drugs are converted into more polar forms by adding functional groups.
- Phase II: Drugs that fail to become excreted after phase I are conjugated into more polar forms.
Without this function, toxic levels of the medications would remain in the bloodstream. Phase I reactions usually involve the microsomal protein CYP450 as well as other microsomal enzyme systems. Phase II usually involves conjugation reactions that are catalyzed by transferases. Substrates for these conjugation reactions usually include the endogenous substances glucuronic acid, sulfuric acid, acetic acid and some amino acids.
Drug-Induced Liver Injury

As mentioned previously. The liver serves as a passageway of almost all the substances that are absorbed from the gut into the circulation. Although processes that happen in the liver in this sense involve the biotransformation of medications and other substances into usable and disposable forms by the organ, this may not be always the case.
Certain medications and harmful substances are actually converted into active toxins once they pass through the liver. An example of which is a drug that is absorbed by the gut as a hapten which could bind to proteins in the liver to cause immunogen production. These newly formed substances can cause hypersensitivity reaction that could ultimately damage many organs and systems, including the liver itself. This is only one of the many mechanisms by which certain medications damage the liver.
Unusual drug reactions leading to acute liver failure commonly develop upon the first exposure to the substance. One can actually draw a diagnosis based from the temporal; relationship between the manifestations and the exposure to the medication.
All over the globe, liver damage caused by drugs are said to happen in 1—14 out of 100,000 individuals. The results from this vary from cases of acute liver failure to more chronic ones. The usually implicated substances for drug-induced liver toxicities include alcohol, herbal medications, dietary supplements, topical medications, toxic chemicals such as fertilizers and pesticides, and of course, over the counter medications such as acetaminophen.
Drug reactions can be characterized as eitherpredictable or idiosyncratic. Predictable drug reactions such as that with acetaminophen are dose-dependent and can mean positive implications in the ease of management. Idiosyncratic reactions usually involve a mixture of cell-damaging processes such as hypersensitivity reactions and direct cytotoxicity. The most commonly affected structures aside from the liver when these reactions happen are the bile ducts. Examples of medications that can trigger these are chlorpromazine and halothane.
As mentioned previously. The liver serves as a passageway of almost all the substances that are absorbed from the gut into the circulation. Although processes that happen in the liver in this sense involve the biotransformation of medications and other substances into usable and disposable forms by the organ, this may not be always the case.
Certain medications and harmful substances are actually converted into active toxins once they pass through the liver. An example of which is a drug that is absorbed by the gut as a hapten which could bind to proteins in the liver to cause immunogen production. These newly formed substances can cause hypersensitivity reaction that could ultimately damage many organs and systems, including the liver itself. This is only one of the many mechanisms by which certain medications damage the liver.
Unusual drug reactions leading to acute liver failure commonly develop upon the first exposure to the substance. One can actually draw a diagnosis based from the temporal; relationship between the manifestations and the exposure to the medication.
All over the globe, liver damage caused by drugs are said to happen in 1—14 out of 100,000 individuals. The results from this vary from cases of acute liver failure to more chronic ones. The usually implicated substances for drug-induced liver toxicities include alcohol, herbal medications, dietary supplements, topical medications, toxic chemicals such as fertilizers and pesticides, and of course, over the counter medications such as acetaminophen.
Drug reactions can be characterized as eitherpredictable or idiosyncratic. Predictable drug reactions such as that with acetaminophen are dose-dependent and can mean positive implications in the ease of management. Idiosyncratic reactions usually involve a mixture of cell-damaging processes such as hypersensitivity reactions and direct cytotoxicity. The most commonly affected structures aside from the liver when these reactions happen are the bile ducts. Examples of medications that can trigger these are chlorpromazine and halothane.
Overview: Acetaminophen
 Image: “Structure of N-acetyl-p-aminophenole (paracetamol or acetaminophen)”
Among the drugs that produce predictable toxic reactions with the liver is acetaminophen. It is considered as the most common cause of acute liver failure with indications of liver transplantation in the United States. Being readily available as an over-the-counter drug, acetaminophen is frequently used inappropriately.
Image: “Structure of N-acetyl-p-aminophenole (paracetamol or acetaminophen)”
Among the drugs that produce predictable toxic reactions with the liver is acetaminophen. It is considered as the most common cause of acute liver failure with indications of liver transplantation in the United States. Being readily available as an over-the-counter drug, acetaminophen is frequently used inappropriately.
Image: “Structure of N-acetyl-p-aminophenole (paracetamol or acetaminophen)”
Among the drugs that produce predictable toxic reactions with the liver is acetaminophen. It is considered as the most common cause of acute liver failure with indications of liver transplantation in the United States. Being readily available as an over-the-counter drug, acetaminophen is frequently used inappropriately.
MECHANISM OF DAMAGE
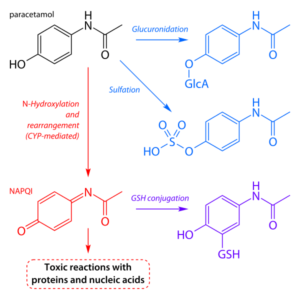 Image: “Simplified schematic of the key pathways of paracetamol metabolism in the human body. The first step in conversion of paracetamol to NAPQI has been omitted for clarity.”
Acetaminophen is commonly used for the treatment of fever and mild pain. It is available in many preparations including tablets, suspensions, syrups, suppositories and intravenous solutions. When taken with a therapeutic dose, most of the acetaminophen is metabolized via conjugation by phase II enzymes in the liver. In the urine, you may find the metabolites of this drug bound to glucuronates and sulfates. However, a small amount of the dose actually escape the phase II conjugation and enter other metabolic reactions that are mediated by CYP proteins. This results in the conversion of otherwise harmless acetaminophen metabolites into N-acetyl-p-benzoquinoneimine or NAPQI.
Individuals who take acetaminophen in proper amounts may be spared from the harmful effects of NAPQI metabolites because these reactive substances can be actually neutralized by conjugation with glutathione. After all, only about 5 % of the total dose enter this type of reaction which could only mean that only traces of NAPQI exist with therapeutic doses.
However, in patients who have taken acetaminophen in large doses as an accident or deliberately for suicide attempts, levels of NAPQI may reach dangerous amounts and start to cause manifestations in the liver. The unconjugated NAPQI metabolites cause hepatocellular injury and ultimately, centrilobular necrosis. This is made possible through 2 mechanisms:
Image: “Simplified schematic of the key pathways of paracetamol metabolism in the human body. The first step in conversion of paracetamol to NAPQI has been omitted for clarity.”
Acetaminophen is commonly used for the treatment of fever and mild pain. It is available in many preparations including tablets, suspensions, syrups, suppositories and intravenous solutions. When taken with a therapeutic dose, most of the acetaminophen is metabolized via conjugation by phase II enzymes in the liver. In the urine, you may find the metabolites of this drug bound to glucuronates and sulfates. However, a small amount of the dose actually escape the phase II conjugation and enter other metabolic reactions that are mediated by CYP proteins. This results in the conversion of otherwise harmless acetaminophen metabolites into N-acetyl-p-benzoquinoneimine or NAPQI.
Individuals who take acetaminophen in proper amounts may be spared from the harmful effects of NAPQI metabolites because these reactive substances can be actually neutralized by conjugation with glutathione. After all, only about 5 % of the total dose enter this type of reaction which could only mean that only traces of NAPQI exist with therapeutic doses.
However, in patients who have taken acetaminophen in large doses as an accident or deliberately for suicide attempts, levels of NAPQI may reach dangerous amounts and start to cause manifestations in the liver. The unconjugated NAPQI metabolites cause hepatocellular injury and ultimately, centrilobular necrosis. This is made possible through 2 mechanisms:
- The unconjugated metabolites bind with the proteins in the hepatocytes, inactivating their cell membrane and mitochondria
- Depletion of glutathione, putting the hepatocytes at an increased risk for oxidation by free radicals (aside from conjugating reactive NAPQI, glutathione also acts as a potent reductant to reactive radicals as well)
A particularly narrow therapeutic window for acetaminophen occurs with alcoholics because alcohol is known to induce the pathways that lead to the conversion of acetaminophen metabolites to NAPQI. This means that alcoholics should be monitored closely when taking this seemingly harmless over-the-counter drug.
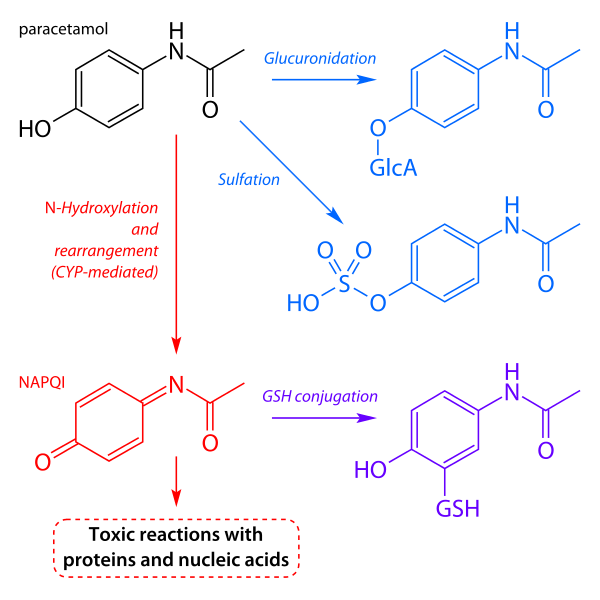
Image: “Simplified schematic of the key pathways of paracetamol metabolism in the human body. The first step in conversion of paracetamol to NAPQI has been omitted for clarity.”
Acetaminophen is commonly used for the treatment of fever and mild pain. It is available in many preparations including tablets, suspensions, syrups, suppositories and intravenous solutions. When taken with a therapeutic dose, most of the acetaminophen is metabolized via conjugation by phase II enzymes in the liver. In the urine, you may find the metabolites of this drug bound to glucuronates and sulfates. However, a small amount of the dose actually escape the phase II conjugation and enter other metabolic reactions that are mediated by CYP proteins. This results in the conversion of otherwise harmless acetaminophen metabolites into N-acetyl-p-benzoquinoneimine or NAPQI.
Individuals who take acetaminophen in proper amounts may be spared from the harmful effects of NAPQI metabolites because these reactive substances can be actually neutralized by conjugation with glutathione. After all, only about 5 % of the total dose enter this type of reaction which could only mean that only traces of NAPQI exist with therapeutic doses.
However, in patients who have taken acetaminophen in large doses as an accident or deliberately for suicide attempts, levels of NAPQI may reach dangerous amounts and start to cause manifestations in the liver. The unconjugated NAPQI metabolites cause hepatocellular injury and ultimately, centrilobular necrosis. This is made possible through 2 mechanisms:
- The unconjugated metabolites bind with the proteins in the hepatocytes, inactivating their cell membrane and mitochondria
- Depletion of glutathione, putting the hepatocytes at an increased risk for oxidation by free radicals (aside from conjugating reactive NAPQI, glutathione also acts as a potent reductant to reactive radicals as well)
A particularly narrow therapeutic window for acetaminophen occurs with alcoholics because alcohol is known to induce the pathways that lead to the conversion of acetaminophen metabolites to NAPQI. This means that alcoholics should be monitored closely when taking this seemingly harmless over-the-counter drug.
MANAGEMENT OF OVERDOSAGE
Initially, efforts to keep the drug from being absorbed in the intestines are instituted. Measures such as induced vomiting, gastric lavage and administration of activated charcoal or cholestyramine are initiated. Other supportive measures are started as well. It is important to flush out any remaining acetaminophen in the stomach by implementing the first two management techniques before administering other medications. However, the time from ingestion should be noted upon admission because some treatments such as the administration of charcoal and cholestyramine become inefficient after 30 minutes from acetaminophen overdosage.
In instances where there is already an increased plasma acetaminophen level (> 200 µg/mL at 4 hours or > 100 µg/mL after 8 hours), N-acetylcysteine may be given. This medication neutralizes the reaction by donating sulfhydryl donor groups to make the used up glutathione molecules available again. This subsequently reduces the incidence of hepatocellular necrosis. However, some patients may still maintain an elevated amount of acetaminophen in the plasma despite N-acetylcysteine administration. For acute liver failure in this context, liver transplantation may be the only.
Initially, efforts to keep the drug from being absorbed in the intestines are instituted. Measures such as induced vomiting, gastric lavage and administration of activated charcoal or cholestyramine are initiated. Other supportive measures are started as well. It is important to flush out any remaining acetaminophen in the stomach by implementing the first two management techniques before administering other medications. However, the time from ingestion should be noted upon admission because some treatments such as the administration of charcoal and cholestyramine become inefficient after 30 minutes from acetaminophen overdosage.
In instances where there is already an increased plasma acetaminophen level (> 200 µg/mL at 4 hours or > 100 µg/mL after 8 hours), N-acetylcysteine may be given. This medication neutralizes the reaction by donating sulfhydryl donor groups to make the used up glutathione molecules available again. This subsequently reduces the incidence of hepatocellular necrosis. However, some patients may still maintain an elevated amount of acetaminophen in the plasma despite N-acetylcysteine administration. For acute liver failure in this context, liver transplantation may be the only.



























0 Comments: